
The Future of Metformin for Prediabetes
By Eliza SkolerKarena Yan
 By Eliza Skoler, Karena Yan, and Kelly Close
By Eliza Skoler, Karena Yan, and Kelly Close
Will the medication move from “off label” to standard of care for people at high risk of developing type 2 diabetes?
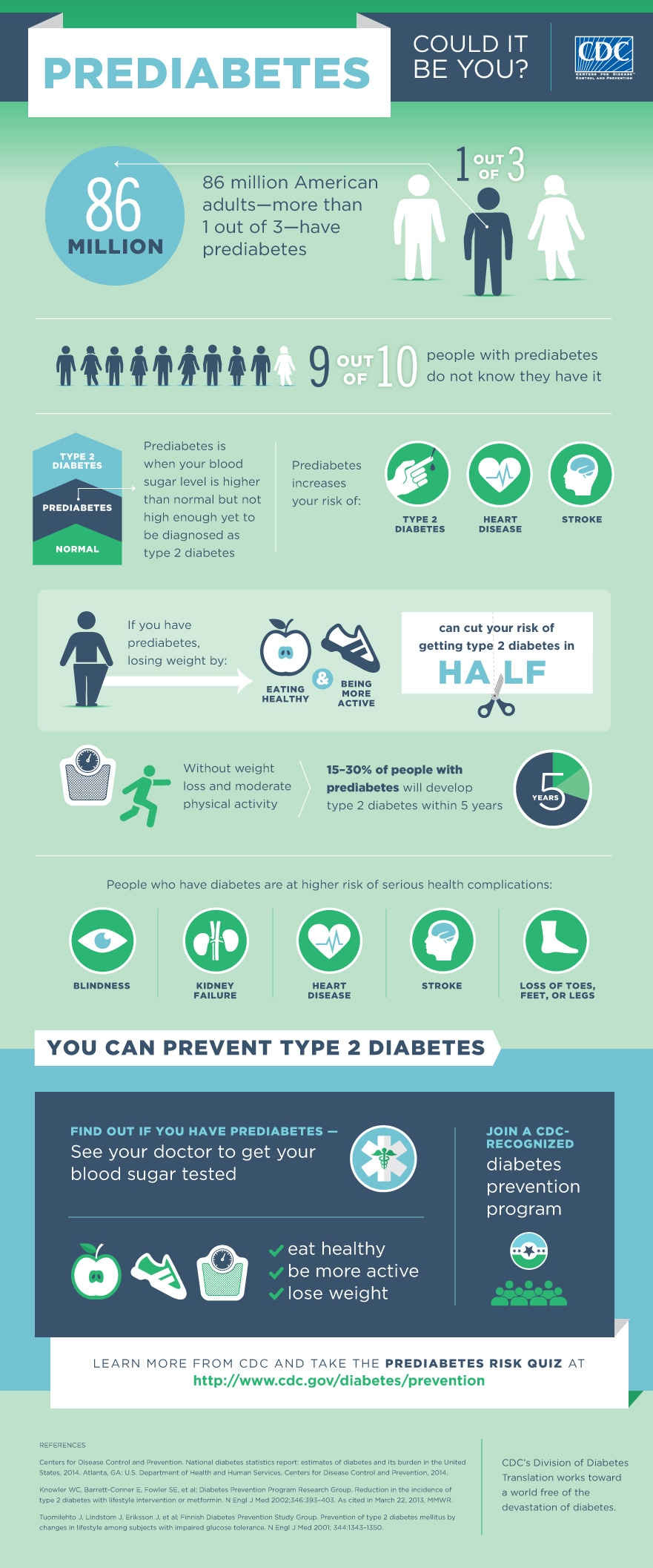
In 2013, we first wrote about the promise of metformin for delaying or preventing the progression of prediabetes to type 2 diabetes. Since then, while the number of Americans with prediabetes has increased from 79 million to over 84 million (one in three US adults), the FDA has not approved metformin for prediabetes – primarily because no organizations have submitted it for approval.
Prediabetes is marked by elevated glucose levels (or an A1C of 5.7-6.4%) that are not high enough to constitute type 2 diabetes but signify an increased risk for eventually developing it. Up to 30% of people with prediabetes will develop the actual disease within five years, and 70% will develop diabetes within their lifetime. Accordingly, experts predict that by 2050, one in four adults will have type 2 diabetes.
Fortunately, there are ways to prevent or delay progression of prediabetes. Two groundbreaking prevention studies, the Diabetes Prevention Program (DPP) and its 15-year follow-up, the Diabetes Prevention Program Outcomes Study (DPPOS), showed that this can be accomplished through lifestyle changes and metformin. The former study found that a low-calorie diet and 150 minutes per week of exercise reduced the risk of type 2 diabetes by 58% and metformin use reduced the risk by 31%.
Metformin is virtually always the first medication prescribed for type 2 patients because it has few side effects and a low cost. It lowers blood sugar levels by decreasing glucose production and absorption, and increasing the body’s sensitivity to insulin. Metformin is a well-studied, generic drug, and with the proper dosage training for health care providers, it has great potential to be used by a variety of people.
Because not all people with prediabetes will develop diabetes, many experts recommend prescribing metformin only to those at the higher end of the risk spectrum. Based on data from DPP, the American Diabetes Association recommends metformin for people under the age of 60, with a BMI greater than 35, or with a history of gestational diabetes – and especially for people whose rising blood glucose levels do not respond to major lifestyle changes.
However, because the FDA has not approved metformin for people with prediabetes, doctors must work around the system and prescribe it “off label” (for a purpose other than its intended use, which is to treat type 2 diabetes). However, even with this loophole, less than 4% of adults with prediabetes are being treated with metformin. “There is global precedent for treating prediabetes, as both Singapore and the Philippines have approved metformin for that very purpose,” said diaTribe founder, Kelly Close, “I believe it should be appropriate for those at very high risk of type 2 to use metformin, but there is not currently a pathway in the United States for this treatment – we’d like to see that change.”
While the obvious pathway to get metformin approved for prediabetes would be for the manufacturer to submit metformin to the FDA using data from DPP and DPPOS, this has not yet happened. Some argue such a submission would be expensive for the manufacturer, but we’ve heard estimates before that this would likely cost $3-5 million – well below the typical cost of an FDA submission in diabetes. “Metformin’s durability, given the results in DPP-OS, also presents an opportunity for the FDA to set a high standard for prediabetes drugs,” says Dr. Robert Ratner, former Chief Scientific & Medical Officer for the American Diabetes Association, “this would in turn allow them to stave off the flood of applications for a prediabetes indication from much more expensive weight-loss drugs.”
The main reason why a submission has not been made is that the company that holds the patent on metformin, Bristol-Myers Squibb (BMS), moved out of the diabetes field a decade ago and no longer has a stake in metformin’s approval. Seeing as they are the only ones who can submit metformin to the FDA, the process has been unable to move forward. In order to change this, BMS should hand its patent over to the American Diabetes Association and others who could make a submission happen. Metformin is a special case where the typical route to FDA approval may need to be adjusted, but it is a goal worth fighting for!
Currently, two trials – VA-IMPACT and GLINT – are studying the long-term cardiovascular effects of metformin in people with prediabetes. VA-IMPACT is being conducted in the US and has nearly 8,000 participants, and GLINT is ongoing in the UK with nearly 13,000 participants. Both are scheduled to end in 2024. Results from these trials will show whether metformin prevents heart disease in people with prediabetes. If there are positive results, this would strengthen the case to approve metformin for prediabetes and represent another reason for a company focused on prevention to prepare an FDA submission for this new indication.
In 2017, diagnosed diabetes cost $327 billion in the US, which equates to one in seven healthcare dollars. With a retail price around $5-15 per month, metformin is cost-effective for both people with prediabetes and for the healthcare system by avoiding costly diabetes complications in the future. Many second-line therapies for type 2 diabetes (medications if metformin and lifestyle changes are not lowering glucose sufficiently) have retail prices in the $500 - $1,000 per month range; a hospital stay for a heart attack costs around $20,000; dialysis costs an average of $89,000 per year. Diabetes prevention in all its forms – not just metformin – can save lives, dollars, and productivity by averting these costly complications.









{kind=link}