
86 Million Americans – It’s Time to Do Something About Prediabetes
By Kelly Close
.jpg) Twitter summary: Millions of people, billions of dollars – why we can’t ignore FDA drug guidance for #prediabetes any longer
Twitter summary: Millions of people, billions of dollars – why we can’t ignore FDA drug guidance for #prediabetes any longer
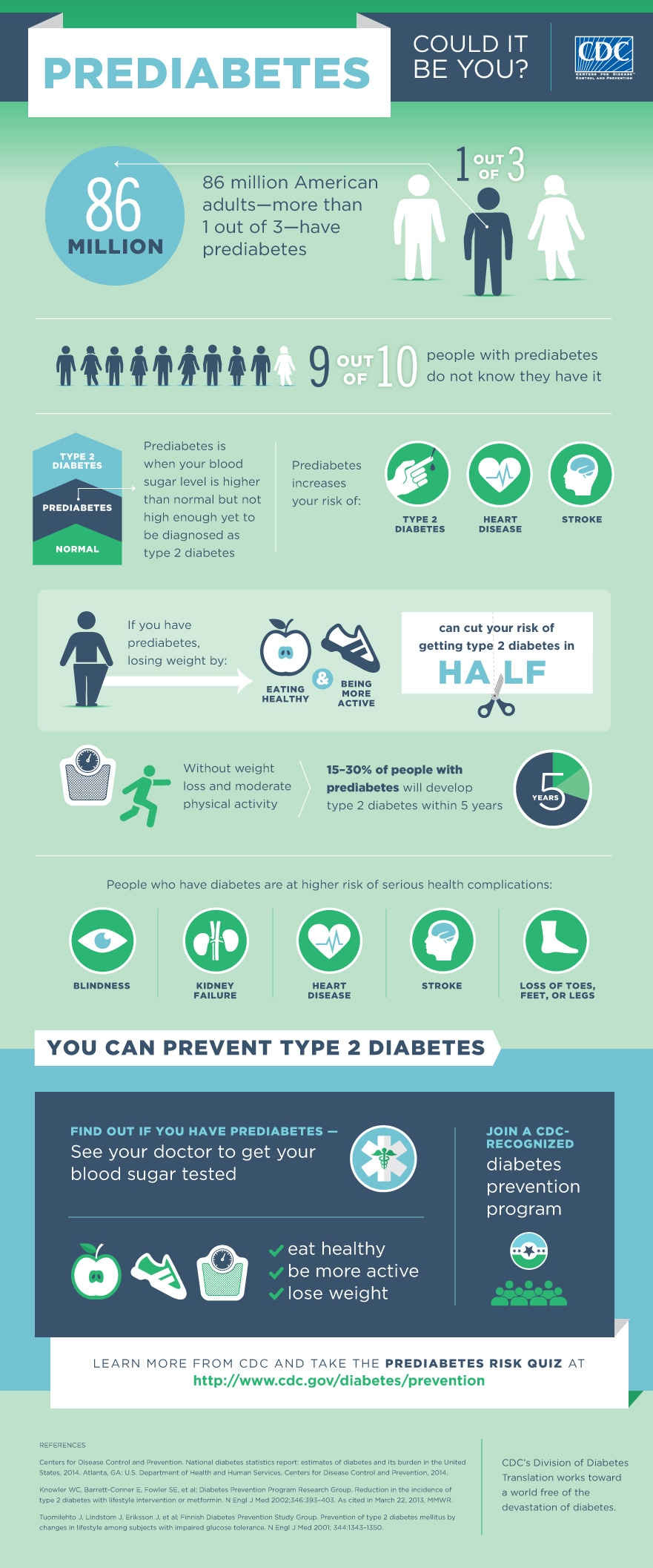
Since I was first diagnosed with diabetes in the mid-1980s, the number of people with prediabetes has nearly doubled to an astounding 86 million Americans today – that’s more than one out of every four people in our country! Prediabetes, which can be diagnosed by having an A1c between 5.7% and 6.4%, is a precursor to type 2 diabetes, and 15-30% of people with prediabetes will develop type 2 diabetes within five years. These numbers mean that as many as 13 to 26 million people with prediabetes will develop type 2 diabetes in the next five years. In other words, the number of type 2 patients in the US could nearly double by 2020. And according to the CDC, 9 out of 10 Americans with prediabetes don’t even know they have it. This means that 77 million people in the US don’t know they have prediabetes and are unknowingly at an increased risk of developing type 2 diabetes. Obviously, this is a huge problem.
A diagnosis of prediabetes can be a wakeup call, an opportunity to reassess one’s lifestyle and make changes. The landmark Diabetes Prevention Program (DPP) study found that lifestyle intervention, including counseling and motivational support on healthy eating, physical activity, and behavior modification, reduced the risk of developing type 2 diabetes by 58% for both men and women compared to standard care. This study also found that metformin, the safest first-line therapy for type 2 diabetes, may help delay the onset of type 2 diabetes in people with prediabetes. Participants in the DPP who did not receive intensive lifestyle intervention but took metformin had a 31% reduced risk of developing type 2 diabetes. Data presented at the ADA 2014 conference showed that after 15 years of follow-up, the results still remained strong: 27% of those in the original lifestyle group had a significant reduction in type 2 diabetes progression, as did 17% of those in the original metformin group. That is pretty incredible for a simple daily pill.
Metformin first came to the US in 1994, and it is estimated to be the most prescribed diabetes medication worldwide. It is safe, cheap, and well-studied, and some clinical evidence suggests it may even reduce the risk of heart disease and cancer. Metformin is often the first drug prescribed for type 2 patients, but it is currently not common practice to prescribe metformin to treat prediabetes – it must be prescribed off-label, since it is not “approved” to treat prediabetes. It’s disappointing to know so many millions of people are not getting access to a potentially life-saving treatment. We do commend the CDC’s National Diabetes Prevention Program’s (NDPP) efforts on lifestyle intervention treatments, self-management education, and more. Unfortunately, though, Medicare will not cover diabetes self-management education and support for people with prediabetes, even though 50% of people 65 and older have prediabetes.
In addition to metformin, there has also been promising prediabetes data from the recently approved GLP-1 agonist Saxenda. In clinical trials, participants with prediabetes on Saxenda were more likely to revert to normal glucose levels (meaning no diabetes or prediabetes at all!) after one year compared to those on placebo (69% of participants on Saxenda vs. only 33% on placebo). The FDA chose not to include this compelling data in Saxenda’s label, meaning providers and patients may not be aware of these benefits.
Why isn’t metformin, or any other drug for that matter, approved for prediabetes? Well, that’s a complicated topic, but one major factor is that the FDA currently doesn’t have any drug guidance whatsoever on prediabetes, which means that it’s very unlikely for drug and device companies to work on any prediabetes treatments. What FDA calls “guidance documents” are extremely valuable for companies looking to develop a drug – they explain what the FDA’s current thinking on a disease area is, and what trials and evidence they want to see in order to approve a drug. Though companies must always work with the FDA to come to an agreement on clinical trial designs, a guidance document lays the groundwork and (at least ideally!) gets everyone on the same page. As of now, no company is making prediabetes drugs for the US, insurance coverage for prediabetes is lacking, and there is very little marketing and public awareness around prediabetes by companies (though some amazing work by the NDPP, ADDE, and others). While this is a multifaceted problem missing clear coordination, the lack of a guidance document represents one straightforward factor that may be deterring companies from pursuing prediabetes. (Indeed, two recently approved obesity drugs, Qysymia and Saxenda, had promising prediabetes data but the data isn’t available on the prescription label for either drug).
A Diabetes Care study published late last year showed that the economic burden of prediabetes rose by 74% to $44 billion between 2007 and 2012. Costs are skyrocketing, and while greater education and lifestyle intervention during prediabetes are absolutely needed treatments, we also need more movement toward drug treatments for prediabetes as well. Of course, it goes without saying that intensive lifestyle intervention is very important and should be reimbursed better than it currently is. That said, we believe a variety of alternatives should be available, and drugs are currently not an option at all in the US - we believe certain compounds should be available to the highest risk individuals with prediabetes. I believe an official FDA guidance document for prediabetes drugs is a logical and productive first step.
So what should happen? Well, let’s learn from those around us! Last year, recognizing a similar need, Parent Project Muscular Dystrophy (PPMD) drafted a guidance on Duchenne muscular dystrophy to help accelerate development and review of potential therapies for this rare disease. This is an amazing effort, and I would love to see the diabetes community discuss how we can learn from PPMD’s example. Certainly our therapeutic areas are very different – but the intent to help the respective fields move forward faster is the same. As we learn more about best ways to collaborate with the FDA, we look forward to working on better guidances and methods to accelerate innovation. If you are interested in prediabetes or have thoughts on an FDA guidance, please say the word – diaTribe.org would love to collaborate.
very best,

Kelly L. Close







{kind=link}