
Expand Your Knowledge of Diabetic Macular Edema (DME)
By Nancy Liu
Twitter summary: Treatments, prevention, and tips for diabetic macular edema (DME).
In our interview with Dr. Michael Cooney of the Vitreous-Retina-Macula Consultants of New York, we talk about diabetic macular edema (DME), treatments available, and three simple steps everyone can take to prevent DME.
What is diabetic macular edema (DME)?
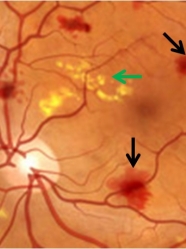
Diabetic macular edema (DME) is a form of diabetic retinopathy where high blood glucose levels can cause leakage and swelling of the macula, a part of the eye responsible for sharp and detailed vision. Over time, damaged blood vessels leak fluid into the macula and cause blurry vision that could eventually lead to blindness. DME affects people with type 1 and type 2 diabetes. Unfortunately, up to 75,000 new cases of DME develop each year in people with diabetes, and it is the leading cause of blindness among working-age Americans. However, there are now several treatment options available and everyone can take simple steps to help prevent or delay DME.

Often, the central vision of people with DME slowly declines over time, and there may be warning signs or symptoms (i.e., blurred vision, floaters, vision loss). Detecting DME early during a retina eye exam and before symptoms develop is the best way to prevent vision loss.
How can DME be prevented?
|
Three Key Tips for Preventing DME |
|
1. Know the vital numbers: blood sugars, blood pressure, and weight. |
|
2. Talk to a health care professional before there is a problem. The best way of preventing complications is being proactive about your risks and having a conversation with your provider before you experience symptoms. |
|
3. Remember to have an annual retina (dilated) eye exam. The exam to check for DME is simple and involves checking vision, eye pressure, and dilating your eyes (which usually wears off after 4 hours). Dr. Cooney recommends everyone with diabetes get a dilated eye exam at least once a year. |
Although there are now more treatments available for DME, the best treatment is always prevention and close monitoring of blood pressure, blood sugars, and weight, although unfortunately this is not always a guarantee. Dr. Cooney illustrated the importance of lifestyle changes together with medical treatment by saying, “[if] you’re stepping on the gas pedal as I’m stepping on the brake, then we’re not going to get very far.”
Another issue has been the lack of awareness and education about DME among patients and providers. A recent survey of people with type 1 and type 2 diabetes from Diabetic Connect found that almost one in four people do not receive the recommended annual retina eye exam. More than half of those surveyed didn’t know DME is a leading cause of vision loss for people with diabetes, and many said they did not know they needed an exam or never talked to their health care provider about vision loss from diabetes.
Dr. Cooney pointed out that there is little communication between primary care physicians, endocrinologists, and ophthalmologists, and the current system must improve education and awareness of DME among providers as well as patients. Patients can request doctors to talk to each other, ask questions, be informed, and check on the status of their health and eye condition.
What treatments are available for DME?
The standard treatment for diabetic macular edema for the past 25 years has been laser surgery, which seals up the leaking blood vessels to reduce the fluid around the macula. The procedure can stop the progression of vision loss but cannot reverse damage that has already been done. In studies, laser surgery reduced the risk of moderate vision loss by 50% over three years, but the surgery can also be expensive and cause side effects.
Lucentis (ranibizumab) was approved by the FDA in August 2012, making it the first drug approved for diabetic macular edema. Lucentis is made by Roche’s Genentech and consists of once-monthly micro injections into the eye. The injection helps to decrease the leakiness of blood vessels, and clinical trials show that over two years, treatment with Lucentis allows individuals to read two additional lines on average on an eye chart – a significant improvement. The drug is also generally safe and well-tolerated – Dr. Cooney mentioned that although many people were originally afraid of the injections, they later said that the pain was “underwhelming.” Laser surgery and Lucentis are also used in parallel to maximize outcomes.
Avastin is a similar drug to Lucentis that has been approved for cancer treatment and is sometimes used “off-label” to treat DME if Lucentis is not available. It may be cheaper than Lucentis, but its safety and effectiveness have not been thoroughly investigated and approved for the treatment of DME.
Steroids are also used off-label to treat DME, although Dr. Cooney warned that these are used as a line of last resort, because treatment can cause additional cataracts and glaucoma.
Resources
For more information on DME and other complications of diabetes and the eye, you can visit Diabetes Eye Check. For a Kerri Sparling’s personal experience dealing with complications and diabetic macular edema, please read our current SUM musings column.
The information published in diaTribe is not a substitute for medical advice and should not be used to make decisions that change treatment. We urge readers to consult with professional healthcare providers for questions regarding their treatment and in all matters related to their health.






