
Dr. George Eisenbarth

For this issue, diaTribe had the opportunity to talk with Dr. George Eisenbarth, the recipient of the Banting Medal for diabetes research-the American Diabetes Association's highest honor. Dr. Eisenbarth's research has laid the foundations for targeted treatment of type 1 diabetes. His Banting lecture was captivating-hundreds and hundreds of people packed the room, eagerly awaiting his words. Not very many of the medals have been given out for type 1 research in recent years, so we were pretty excited about this. He reviewed the current state of type 1 research and therapies available for preventing type 1, but most importantly he talked about the possible path to prevent type 1 diabetes.
The most uplifting and promising part of his talk was that the “tipping point”--the ability to prevent type 1--is near. It all depends on a “trimolecular complex” discovered in mice that explains the details of how a person's immune system is responsible for starting down the disease path. The formation of this “trimolecular complex,” (which Dr. Eisenbarth discovered) involves the improper activation of the immune system's 'attack cells' (T-cells). These attack cells activate pathways that destroy beta cells, the pancreatic cells that produce insulin. Ultimately, this leads to type 1 diabetes. Dr. Eisenbarth is now working on drugs that would prevent type 1 in mice and is looking to see if this all works the same way in humans.
In this interview, Dr. Eisenbarth discusses how his discoveries can move us towards preventing diabetes and what they mean for diagnosing and predicting the disease.
diaTribe: Thank you so much for being with us, Dr. Eisenbarth. We were thrilled to hear you deliver the Banting Lecture at this year's ADA Meeting. What a thrill for people with type 1 that type 1 diabetes was the focus of the lecture. After so many years of hearing about a cure, it is wonderful to hear we really are getting much closer. Can you tell us a little about when you were asked to give the lecture and a little bit about the process of putting together the Banting Lecture, the most prestigious lecture to deliver in all of diabetes?"
Dr. Eisenbarth: I was obviously very pleased in particular for the opportunity to share thoughts on a pathway for prevention of diabetes. It was the most formal talk I have ever given, with help from the ADA and hours of practice with a TelePrompter, something that, as a physician scientist, I've never used before.
 the biology of diabetes
the biology of diabetes
diaTribe: So let's hit the science straightaway! Could you explain to us in a little more detail what happens at the cells and molecules level in type 1 diabetes?
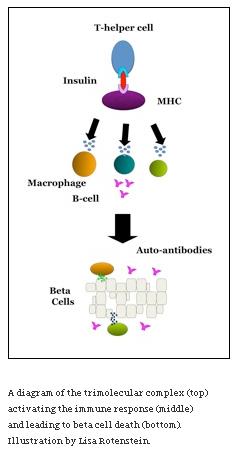
Dr. Eisenbarth: Humans are born with the ability to form the trimolecular complex. This complex consists of an attack cell (T-cell) receptor, the insulin molecule, and a molecule presented on all of a person's cells called MHC [the molecule presents “pieces” of our cells for recognition by the immune system]. This complex is formed in normal immune reactions as well, but in those cases either 1) the immune response is against a foreign molecule, rather than a person's own molecule (like insulin), or 2) attack cells are ones which stifle immune responses rather than trigger them.
When this trimolecular complex forms with an insulin molecule, as it does in diabetes, it means that our bodies are recognizing insulin as foreign and so telling attack cells to attack our beta cells (because they produce insulin).
In the case of type 1 diabetes, fairly ubiquitous environmental triggers change the T-cells from stifling to attacking and cause this complex that shouldn't form to form. It's like having a match in a matchbox. You always have the ability to light it, but that doesn't mean it's always lit-something has to set it off. We now know multiple viruses can do this. We've seen cases where if you administer virus to animals, three to four weeks later they get diabetes or have diabetes.
I believe the triggers are likely very common and are many of the infections that we're ordinarily exposed to during our lives. The triggers are really what ultimately start autoimmunity-when they take place, you start producing auto-reactive T-cells and auto-antibodies against beta cells-the hallmark of type 1 diabetes.
predicting diabetes
diaTribe: How does this help us predict who will get diabetes?
Dr. Eisenbarth: One clue we have is that antibodies are predictive of progression to diabetes. Once a person has multiple auto-antibodies, that person is almost certainly progressing towards disease, even though that progression may take years. Genes could be the key to predicting the time of progression for people who already have antibodies. It's also important to know that antibodies can appear at any age, not just in childhood.
Another clue is whether a person has protective HLA molecules. This type of molecule is seen on the surface of immune cells involved in the diabetes autoimmune response. Twenty percent of us carry these. Only 1% of individuals who develop diabetes carry them.
diaTribe: What we've talked about so far was discovered in mice and the treatment strategies are still in mice. How does this translate into humans?
Dr. Eisenbarth: We assume that man has a similar complex because humans have diabetes. But we haven't yet identified the components in man. Because of work we're doing in my lab, we'll know in the next few months if what determines the immune response in mice and humans is the same. [Once this is known, this will help with translating treatments designed for mice into humans].
prospects for treating type 1 diabetes
diaTribe: How does our new understanding of type 1 diabetes autoimmunity help us better treat the disease?
Dr. Eisenbarth: This knowledge gives us lots of new targeted options for treatment. The first approach involves blocking formation of the complex we've been talking about so that the autoimmune reaction never starts. We are working on creating small molecules that can do this.
“Vaccination” against the complex is another exciting choice. We are trying to generate antibodies to the complex so that the immune system knows to destroy it. We're testing this concept in mice right now.
The one million people in the US developing type 1 diabetes typically show antibodies before developing diabetes, and so with these kinds of approaches, you could administer treatment to keep them non-diabetic [and prevent the disease].
diaTribe: What's the outlook for people who have had diabetes for 25 or 30 years now that we have this insight?
Dr. Eisenbarth: None of the approaches I talked about would work in these patients. By this point, all of their beta cells would probably have been killed. Nevertheless, we need to prevent the autoimmune killing for islet transplantation procedures or stem cell replacement of islets intended to cure diabetes [otherwise islets or stem cells are destroyed by our bodies].
The approaches we're talking about are all about prevention-specifically about antibodies and T-cells. The antibodies are what cause diabetes' effects. If we can prevent antibody formation or survival, we can help prevent beta-cell failure.
diaTribe: So from what I'm understanding, all of this means that type 1 diabetes doesn't necessarily just have to be a juvenile disease? Whenever the environmental trigger happens, the complex forms, antibodies are created, and diabetes symptoms can start?
Dr. Eisenbarth: Probably half of type 1 diabetes occurs after age 40 and there's a second peak of type 1 diabetes incidents in the 70s, the 80s. At our center, when an adult presents with typical type 2 diabetes, we make sure we measure auto-antibodies. If they have one or more types of auto-antibodies, they very likely have type 1 diabetes. In that case, it's important to start them on insulin therapy much earlier because this could help preserve their beta cells.
We thought Dr. Eisenbarth’s work and his Banting Lecture have huge implications for the field. What does it all mean? We hope that eventually, if a person presents with auto-antibodies, doctors will be able to treat them in a way that stops the progression of their diabetes and the death of their beta-cells. This will take time--time to translate mouse work to humans and time to develop new drugs. Maybe we’ll be able to identify the environmental triggers and have patients who are genetically susceptible to diabetes avoid them. And in the meantime--it makes us smarter and gives direction so we can be specific in designing therapies.
We’d also like to put in a plug for patients to get their antibodies checked if they’ve been recently diagnosed with type 1 or are first degree relatives of patients with type 1. TrialNet, at www.diabetestrialnet.org, is a wonderful resource that is conducting trials related to the prevention and early diagnosis of type 1 diabetes.






